- Preventive healthcare lowers long-term treatment costs and improves workforce productivity.
- Rising chronic diseases make prevention a strategic priority for India.
- Screenings, vaccinations, and early detection reduce healthcare burden.
- Technology can scale preventive healthcare to underserved regions.
- Smile Foundation advances preventive healthcare through Smile on Wheels outreach.
Prevention is better than cure. Cliché as the saying may be, it remains deeply relevant today. Preventive care is preferable to curative care because it is the first step towards protecting your health by stopping a problem before it begins.
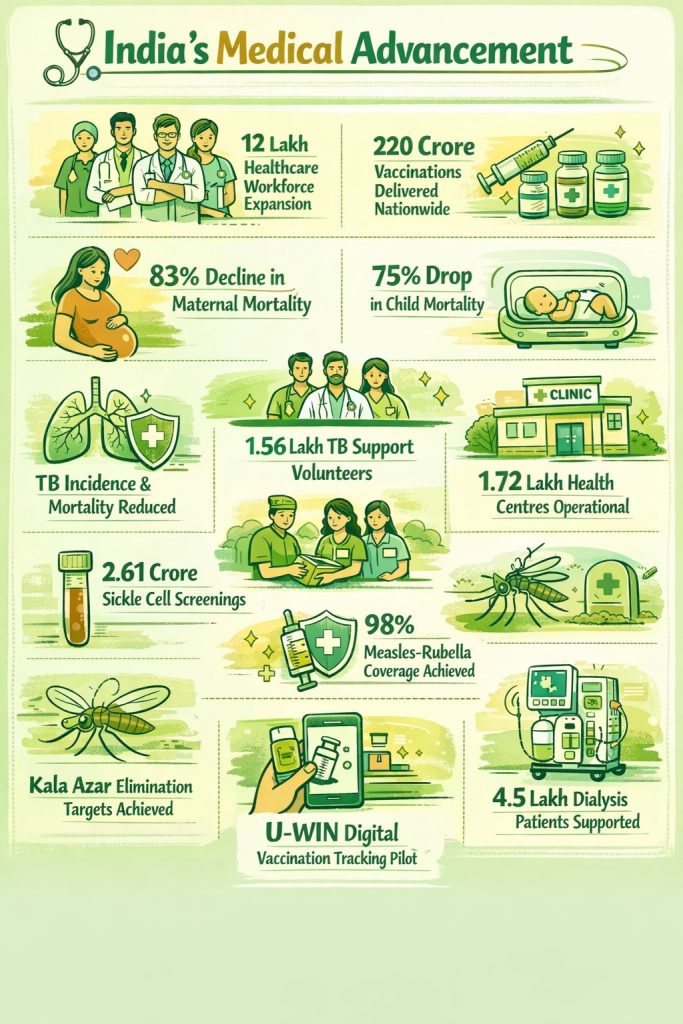
Over the past few decades, India’s healthcare sector has undergone a significant transformation, driven by advances in infrastructure, technology, and accessibility. The country’s reputation as a leading destination for medical value travel reflects both the quality of its healthcare services and the strength of its branding. Yet heart disease, diabetes, and cancer continue to rise, often affecting Indians earlier in life, especially those outside urban centres. Most people see a doctor only when symptoms become hard to ignore. What is the use of a system that is so advanced, but is built to treat and does too little to prevent?
Preventive Healthcare System the Need of the Hour
It’s simple: every penny spent treating preventable chronic disease is money that could be used elsewhere in the health sector. Shifting to a prevention-focused ecosystem would bring major benefits, including longer healthy life expectancy, lower health inequalities, fewer hospitalisations, and more fulfilling, productive lives in which people can participate fully in their communities, education, and work. Higher productivity would also strengthen GDP.

What Prevention Really Means
Preventive healthcare offers a different path. It focuses on action before symptoms appear. It includes routine screenings, vaccinations, early risk detection, and lifestyle changes. It also recognises that health risks do not look the same for everyone.
This is where genetics and family history also enter the conversation. If diabetes runs in your family, your risk starts higher. If close relatives have had cancer or heart disease, your screening timeline should begin earlier. Prevention, in this sense, is then targeted, informed, and continuous.
Broadly, preventive healthcare includes:
· Regular screenings for cancers like breast, colorectal, cervical, and prostate tests that can spot problems before they become serious.
· Routine checks for blood pressure, cholesterol, and diabetes help flag metabolic conditions that, if ignored, could lead to major complications down the line.
· For those entering or past menopause, osteoporosis screenings help detect bone loss before fractures occur.
· Vaccines also play a big part, including annual flu shots and other immunisations tailored to your age, travel plans, or health history.
· Counselling on things like quitting smoking, mental health, and healthier lifestyle choices. Even screenings for certain sexually transmitted infections fall under this umbrella, depending on your age and risk factors.
Why India Cannot Wait
The urgency of this shift becomes clear when you look at India’s disease profile, lifestyle, and culture.

As chronic diseases rise and healthcare costs soar, the urgency to reorient from treating sickness to proactively preventing it has never been greater.
What Needs to Change?
Make Preventive Care Accessible and Affordable
To truly shift from curative to preventive healthcare, we have to focus on making preventive services easy to access and affordable for everyone. This means that routine screenings should be an integral part of everyday primary care and supported by insurance.
Embrace Technology for Better Access
Technology is another game-changer. With tools like telemedicine, wearable health trackers, and digital health records, we can keep an eye on health risks as they arise and bridge the access gap for folks living in remote areas.

Rethink Awareness Campaigns
Awareness campaigns need to ditch the generic messaging and connect with people on a personal level, addressing their real lives, cultures, habits, and risks. By tapping into schools, workplaces, and community networks, we can reinforce these messages and make prevention feel much more personal.
Strengthen Health Data Systems
India also needs robust health data systems. Good data helps spot patterns, predict risks, and focus resources where they matter most.
Redefine the Role of Doctors
A doctor’s role in a patient’s emotional support is worth stressing. Doctors should offer guidance, early detection, and collaborate with nutritionists and therapists.
Build a Collaborative Ecosystem
If we want a healthier future, it will take a collaborative push from educators, employers, NGOs, health innovators, and the government. Empowered individuals, smart legislation, integrated technology and community support can only make prevention the genuine backbone of healthcare.
Going Forward with Preventive Care
Some real-world examples of the most developed preventive health care systems include widespread vaccination programs, lifestyle interventions, early screenings, digital monitoring, and comprehensive public health campaigns. Sweden has long been known for its robust welfare state and emphasis on public health. Preventive health is a fundamental part of the Swedish health care system. Japanese people have one of the longest life expectancies in the world. Singapore has emerged as a world leader in digital health and preventive care.
Smile Foundation has been actively involved in creating awareness among the most vulnerable and poverty-stricken people from the remote corners to urban villages of India. With over 100 “Smile on Wheels”, Mobile Medical Units are growing in underserved communities all over the country to strengthen access to essential primary healthcare services.
FAQs: Shift from Curative to Preventive Healthcare
1. What is preventive healthcare?
Preventive healthcare focuses on avoiding illness before it starts through regular screenings, vaccinations, health check-ups, early risk detection, and healthy lifestyle choices.
2. How is preventive healthcare different from curative healthcare?
Curative healthcare treats illness after symptoms appear, while preventive healthcare aims to reduce the chances of disease developing in the first place.
3. Why does India need to shift towards preventive healthcare?
India faces a growing burden of chronic diseases such as diabetes, heart disease, hypertension, and cancer. Prevention can reduce hospitalisations, lower healthcare costs, and improve quality of life.
4. What are examples of preventive healthcare services?
Examples include blood pressure checks, diabetes screening, cancer screening, vaccination, cholesterol tests, osteoporosis checks, mental health counselling, and tobacco cessation support.
5. Can preventive healthcare reduce medical expenses?
Yes. Detecting risks early often prevents expensive treatments, surgeries, and prolonged hospital stays later, making healthcare more affordable for families and the system.
6. How can technology support preventive healthcare?
Telemedicine, wearable devices, digital health records, and mobile health apps can track health indicators, remind people about check-ups, and improve access in remote areas.
7. What role do doctors play in preventive healthcare?
Doctors guide patients on lifestyle changes, recommend screenings, identify risks early, and work with nutritionists or therapists to support long-term wellness.
8. How are organisations like Smile Foundation supporting prevention in India?
Smile Foundation supports preventive healthcare through awareness campaigns and its Smile on Wheels programme, which delivers essential healthcare services to underserved communities across India.