
Summary
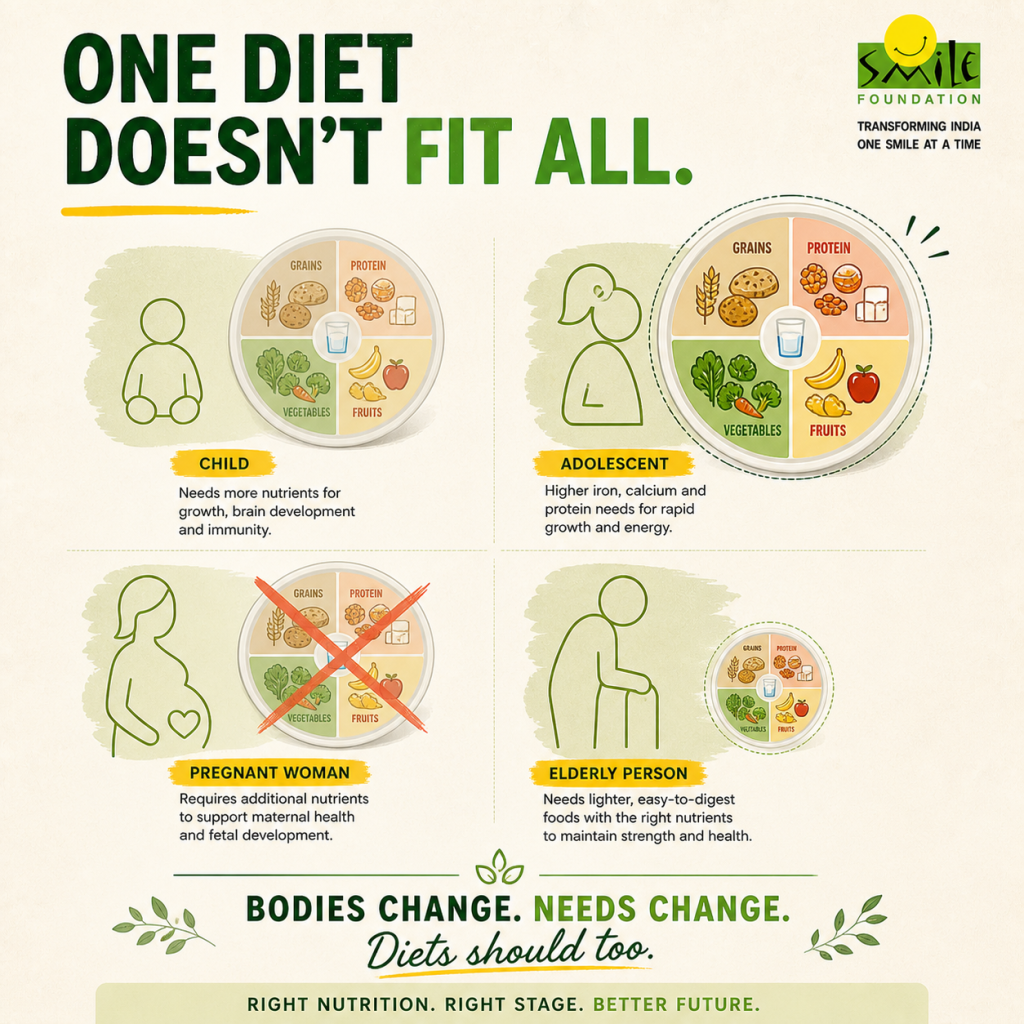
- Nutrition needs evolve from infancy to old age
- One-size-fits-all diets fail across life stages
- Healthcare in India faces stunting, anaemia, undernutrition and obesity
- Global diet trends must suit India’s affordability and food culture
- Life-course nutrition improves health through targeted care and awareness

The idea that there exists a single balanced diet suitable for everyone is one of the most enduring simplifications in nutrition discourse over time. It promises clarity: eat this-avoid that-maintain moderation but obscures a far more complex biological and social reality that human bodies are not static. In fact, they change continuously across the life cycle, shaped by phases of rapid growth, hormonal transitions, reproduction, ageing and shifting patterns of work and care.
Recognising this, organisations such as the World Health Organization, UNICEF and the Food and Agriculture Organisation increasingly advocate for a ‘life-course approach’ to nutrition, one that accounts for these transitions rather than flattening them. Nowhere is this more urgent than in contexts like India, where multiple forms of malnutrition coexist across age groups, from stunted children to anaemic adolescents and undernourished mothers. In such a landscape, the persistence of one-size-fits-all dietary thinking is inadequate and actively limits the effectiveness of nutrition policy and practice.
The very importance of nutrition
During infancy and early childhood, nutrition plays a foundational role in physical growth and cognitive development. The first 1,000 days, from conception to around two years of age, are widely recognised in public health as a critical window. Nutritional deficiencies during this period, particularly in protein, iron, iodine and essential fatty acids, can lead to irreversible consequences such as stunting, impaired brain development, weakened immunity etc., later in life. Applying adult dietary frameworks to children—whether through portion sizes or nutrient composition—would mean ignoring these developmental imperatives.
As children transition into adolescence, the body undergoes another dramatic transformation. Puberty introduces rapid growth spurts, hormonal changes, increased nutritional demands, say how iron requirements rises significantly for menstruating girls. Yet, this stage is often marked by erratic eating habits. Thus, a generalised guideline that does not account for these physiological and behavioral shifts risks exacerbating deficiencies precisely when the body requires heightened support.

Adulthood is frequently treated as the “standard” phase upon which most dietary recommendations are based. However, even within this category, nutritional needs are far from uniform. A sedentary office worker, a manual labourer, a pregnant woman and an athlete all occupy vastly different metabolic realities. Ignoring these distinctions vis-a-vis generic dietary advice can contribute to maternal malnutrition, low birth weight, intergenerational cycles of poor health and other issues.
Read this: https://www.smilefoundationindia.org/blog/first-1000-days-of-a-child/
Why One-Size-Fits-All fails
The failure of one-size-fits-all is not just a biological problem but also a systemic one. Public health programmes, food policies and even commercial diet cultures often rely on generalised frameworks for scalability and simplicity. Such standardisation is often administratively convenient, but overlooks the diversity of human needs. This is why school meal programmes, workplace canteens, elderly care facilities often frequently operate on uniform menus that do not adequately reflect the specific nutritional requirements of their populations and age groups.
Additionally, the rise of global diet trends, such as high-protein regimens, intermittent fasting or calorie-restrictive plans, has further reinforced the illusion of universal applicability. These approaches often emerge from specific cultural and economic contexts but are marketed as broadly effective solutions across populations which is very problematic.
Take, for instance, the so-called Mediterranean diet, which is rooted in particular regional food systems and lifestyles. Its emphasis on olive oil, seafood, lean meats and fresh produce reflects not only nutritional principles but also geographic availability and long-standing cultural habits. Transposing such a diet to the Indian context is not straightforward. Food systems in India are shaped by different climatic conditions, agricultural patterns, and most importantly, socio-economic constraints. Olive oil, for example, is neither locally produced at scale nor affordable for large sections of the population. Also, seafood consumption remains uneven across regions.
When such trends are adopted without accounting for differences in age, health status or local dietary practices, they can do more harm than good. Intermittent fasting, for example, may be unsuitable for adolescents, pregnant women or older adults with underlying health conditions, highlighting the risks of applying generalised diet frameworks to diverse physiological and socio-cultural realities.
Nutrition for All with Smile
An age-specific approach to nutrition, therefore, is not a luxury but a necessity. It requires rethinking how dietary guidelines are framed and implemented. Instead of generic balanced diet models, nutrition policies must incorporate life-stage frameworks that recognise shifting needs. This includes targeted interventions such as fortified foods for children, iron supplementation for adolescent girls, maternal nutrition programmes and specialised diets for the elderly.
Equally important is the role of education and awareness. Individuals and caregivers must be equipped with knowledge that allows them to adapt diets according to age and context. This is
particularly crucial in countries like India, where nutritional challenges coexist across the spectrum, from undernutrition to rising obesity. An age-sensitive approach can help address this ‘double burden’ more effectively than blanket recommendations.
The healthcare system, too, has a critical role to play. Routine nutritional screening at key life stages: adolescence, pregnancy and old age, can shift the focus from reactive treatment to preventive care. Early identification of deficiencies, coupled with timely dietary interventions, can significantly reduce the burden of both malnutrition and non-communicable diseases.
At the end, it is pertinent that we approach nutrition as a dynamic, life-course process and as a life-course priority, not a one-time prescription. An age-specific approach is essential to address India’s dual burden of undernutrition and rising lifestyle diseases through timely care, screening and awareness.
In this direction, Smile Foundation is driving impact through Smile on Wheels, which takes healthcare and nutrition awareness camps to schools and communities, enabling early intervention and informed choices. Through Pink Smile, focused efforts support the nutrition and wellbeing of young girls, women, and infants. Such targeted, preventive models show how community-led action can build healthier generations across every stage of life.
Frequently Asked Questions (FAQs)
1. Why does one-size-fits-all fail in healthcare?
Because human bodies are not uniform. Nutritional needs vary across age, gender, occupation, health status and life stages. A diet suitable for a sedentary adult may be inadequate for a growing adolescent or a pregnant woman. Generic dietary advice overlooks these differences, making it ineffective and, in some cases, even harmful.
2. Why is life-stage nutrition important in healthcare?
Nutritional requirements change significantly from infancy to old age. Each stage—early childhood, adolescence, adulthood, pregnancy and ageing—comes with distinct physiological demands. A life-stage approach ensures that diets are aligned with these changing needs, supporting growth, preventing deficiencies and improving long-term health outcomes.
3. How does poor diet affect children’s healthcare?
Inadequate nutrition during early childhood can have lasting consequences. It can lead to stunting, weakened immunity, delayed cognitive development and reduced learning capacity. These early deficits often carry into adulthood, increasing vulnerability to diseases and limiting overall potential in education and livelihoods.
4. Why is adolescent nutrition important in healthcare?
Adolescence is a period of rapid physical growth and hormonal change, which significantly increases nutritional needs—especially for iron, protein and micronutrients. Poor dietary intake during this stage can result in anaemia, fatigue, reduced physical development and long-term health challenges, particularly for girls.
5. How does balanced diet support maternal healthcare?
Proper nutrition during pregnancy is critical for both the mother and the child. It helps reduce risks such as anaemia, complications during childbirth and low birth weight. A balanced diet supports healthy fetal development, strengthens maternal health and helps break intergenerational cycles of malnutrition.
6. Can global diet trends improve diet and healthcare?
Not always. While global diet trends may offer useful insights, they are often rooted in specific cultural and economic contexts. Without adapting them to local food systems, affordability and individual health needs, such trends can be impractical or even counterproductive, especially in diverse settings like India.
7. What role does preventive healthcare play?
Preventive healthcare shifts the focus from treatment to early detection and intervention. Regular nutritional screening, awareness and counselling help identify deficiencies before they become severe. Timely dietary support can reduce the burden of both malnutrition and lifestyle diseases, improving overall health outcomes.
8. What is the future of India’s healthcare?
The future lies in moving beyond standardised approaches towards more personalised, life-stage-based nutrition strategies. Integrating awareness, regular screening and targeted interventions can help address India’s dual burden of undernutrition and rising lifestyle diseases, building a more responsive and inclusive healthcare system.




