

Summary
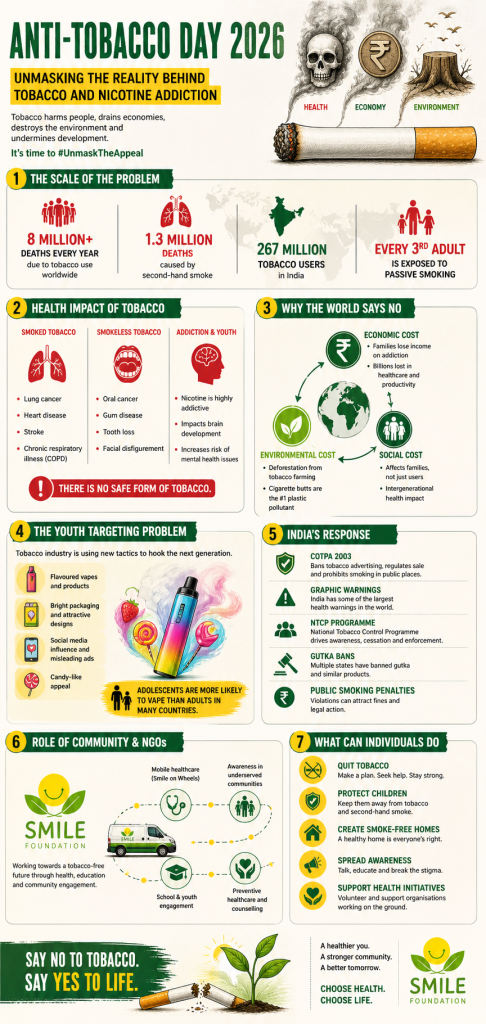
- Tobacco kills more than 8 million people every year globally, including approximately 1.3 million non-smokers who die from second-hand smoke exposure, making it one of the largest preventable causes of death in human history
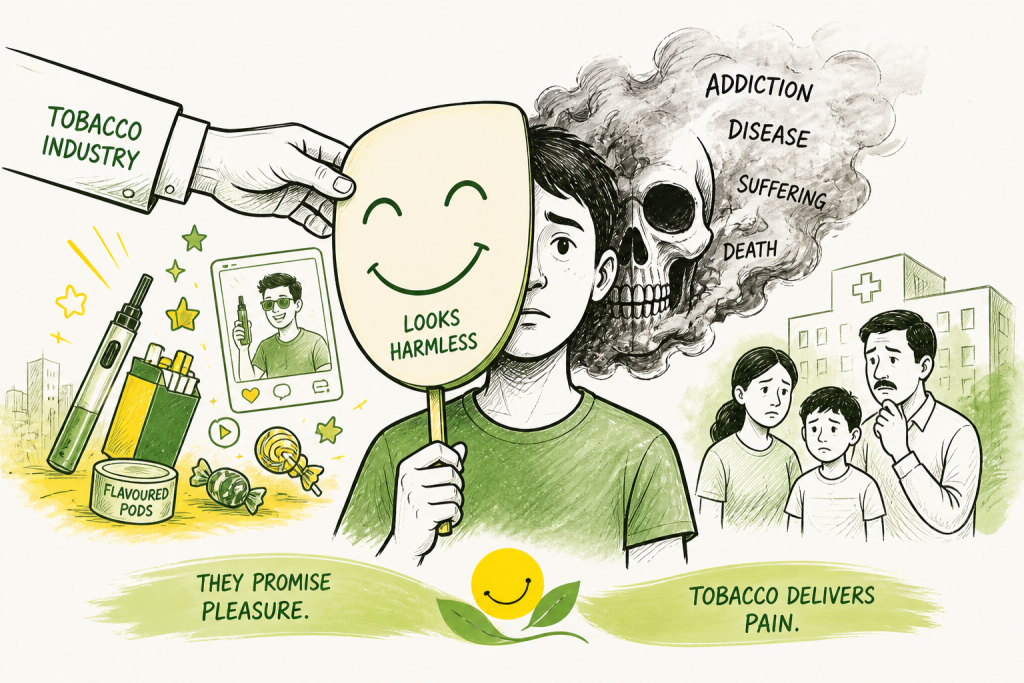
- The WHO’s theme for Anti-Tobacco Day 2026 — Unmask the Appeal: Countering Tobacco and Nicotine Addiction — focuses on how the tobacco and nicotine industry continues to make harmful products attractive, particularly to young people, through flavours, packaging and digital marketing
- India is home to approximately 267 million tobacco users, with tobacco-attributable deaths exceeding one million per year driven by both smoking and widespread smokeless tobacco use, including gutka, khaini and zarda
- India has developed one of the stronger tobacco control frameworks among middle-income countries including COTPA 2003, large pictorial health warnings, the National Tobacco Control Programme, and a ban on e-cigarettes but enforcement gaps and insufficient cessation infrastructure remain significant challenges
- The deliberate targeting of youth by tobacco and nicotine companies through e-cigarettes, nicotine pouches, flavoured devices and social media influencer marketing represents one of the most serious emerging threats in global tobacco control
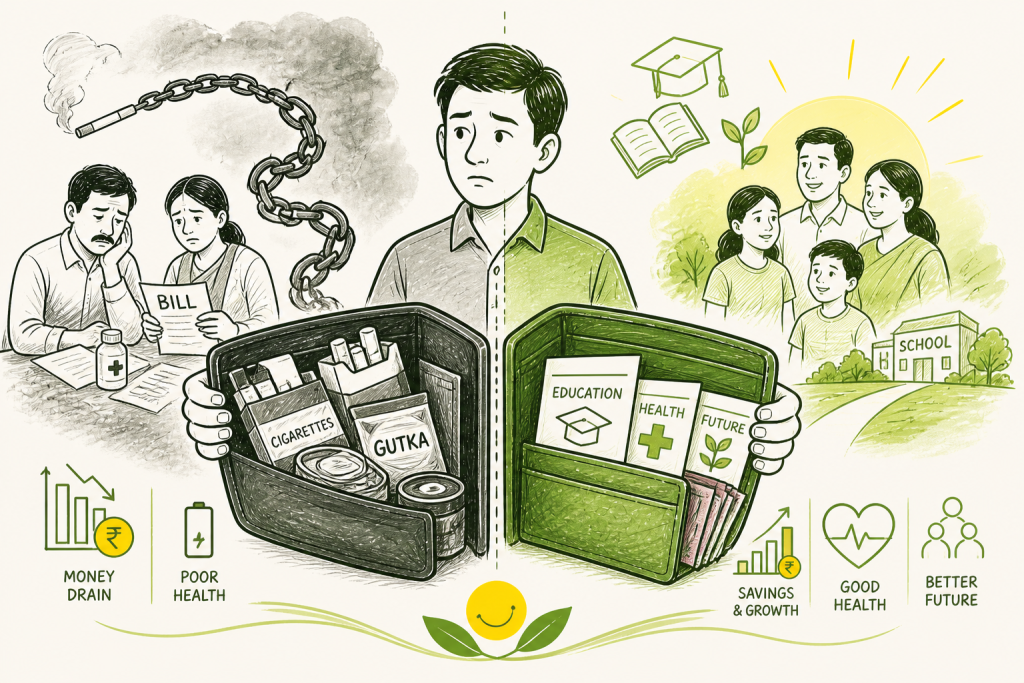
- The socio-economic burden of tobacco is particularly acute in low-income households, where spending on tobacco products competes directly with food, education and healthcare creating a cycle of poverty and addiction that policy alone cannot easily break
- Community organisations and NGOs including Smile Foundation through its Smile on Wheels mobile healthcare programme play an irreplaceable role in extending tobacco awareness, health education and preventive care to populations that national campaigns do not consistently reach
- Quitting tobacco produces measurable health benefits at any age and after any duration of use with cardiovascular risk improving within weeks and cancer risk declining significantly within years making cessation support one of the highest-impact investments in public health
A Habit the World Cannot Afford: Anti-Tobacco Day 2026
Every 31 May, the world pauses to confront one of the most persistent and preventable causes of death in human history. World No Tobacco Day or Anti-Tobacco Day 2026 is not a commemoration. It is a reckoning. A reminder that tobacco, in all its forms, continues to kill at a scale that would be considered a global emergency in any other context.
In 2026, that reckoning feels more urgent than it has in years. Not because tobacco use has surged — in many countries, smoking rates have declined. But because the tobacco and nicotine industry has reinvented itself, found new markets, developed new products and identified a new generation of potential users. The threat has not diminished. It has evolved.
The WHO’s official theme for Anti-Tobacco Day 2026 — Unmask the Appeal: Countering Tobacco and Nicotine Addiction — captures this precisely. It is not enough to warn people about the dangers of smoking. It is necessary to understand how addiction is manufactured, marketed and made to seem normal, and to counter those mechanisms at every level, from national policy to individual conversation.
The Scale of the Problem: What the Numbers Say
Tobacco remains one of the largest preventable causes of death globally. According to the WHO, tobacco kills more than 8 million people every year. Of these, approximately 1.3 million are non-smokers who die from exposure to second-hand smoke — people who made no choice to use tobacco but paid for others’ addiction with their health and their lives.
The economic cost is equally staggering. Global healthcare expenditures attributable to tobacco use run into hundreds of billions of dollars annually. When lost productivity through premature death, chronic illness and disability is factored in, the total economic burden runs far higher. For low- and middle-income countries, which already carry a disproportionate share of the global disease burden, the cost of tobacco is not abstract. It competes directly with investment in education, infrastructure and poverty reduction.
The health consequences of tobacco use are wide-ranging and well-documented. Smoking is strongly associated with lung cancer, chronic obstructive pulmonary disease, cardiovascular disease, stroke and reduced immune function. But the damage is not limited to the lungs or the heart. Tobacco use affects nearly every organ system in the body from the kidneys and the bladder to the bones and the reproductive system. Smokeless tobacco products, which tend to receive less public attention than cigarettes, carry their own serious risks: oral cancer, gum disease, oesophageal cancer and cardiovascular problems. In countries like India, where smokeless tobacco use is widespread, this distinction matters enormously.
India’s Tobacco Landscape: A Complex and Urgent Picture
India’s relationship with tobacco is both large in scale and complex in character. The country is home to approximately 267 million tobacco users — one of the largest tobacco-using populations in the world. What makes India’s situation particularly challenging is the diversity of tobacco consumption patterns. Smoking, in the form of cigarettes and bidis, coexists with a wide variety of smokeless tobacco products, including gutka, khaini, zarda, pan masala mixed with tobacco and snuff. Bidis, which are hand-rolled and typically unfiltered, account for a significant proportion of tobacco consumption and are often perceived, incorrectly, as safer than cigarettes.
The health burden that follows from this is significant. India accounts for a disproportionate share of global oral cancer cases — a direct consequence of high smokeless tobacco use. Cardiovascular disease, chronic respiratory illness and tobacco-related cancers collectively place enormous pressure on a healthcare system that is already stretched. According to estimates, tobacco-attributable deaths in India run to over one million per year. The years of productive life lost to premature death and chronic disability represent a development challenge as much as a health one.
The socio-economic dimension of tobacco use in India deserves more attention than it typically receives. Tobacco consumption is not evenly distributed across income groups. Poorer households spend a higher proportion of their income on tobacco products, creating a cycle in which addiction diverts resources from food, education and healthcare. Research has consistently shown that tobacco expenditure in low-income households competes directly with nutritional spending — a particularly serious concern in a country where malnutrition remains a significant public health challenge.
India’s Policy Response: Significant Steps, Persistent Gaps
India has, by the standards of middle-income countries, developed a reasonably robust legislative framework for tobacco control. The Cigarettes and Other Tobacco Products Act — COTPA — enacted in 2003, remains the central legal instrument. It prohibits smoking in public places, restricts advertising across multiple media, bans tobacco sales near educational institutions and requires health warnings on packaging. These are not trivial provisions. Enforced consistently, they have real potential to reduce consumption and protect non-smokers from second-hand smoke exposure.
India’s pictorial health warnings which cover a significant proportion of tobacco packaging are among the largest in the world. Research on health warning effectiveness consistently shows that graphic, image-based warnings are more effective than text alone, particularly in populations with lower literacy levels. For a country as linguistically diverse as India, images that communicate risk without relying on any single language are an especially important policy tool.
The National Tobacco Control Programme, operating through state-level tobacco control cells and district-level implementation, provides the administrative infrastructure for enforcement, cessation services and public awareness. Recent enforcement actions in states including Karnataka have demonstrated that implementation, where it occurs, does produce measurable results — fines for public smoking violations, crackdowns on illegal sales near schools and removal of tobacco advertising from prohibited areas.
The action taken against specific smokeless tobacco products including state-level bans on gutka and restrictions on pan masala with tobacco under food safety regulations represents a recognition that tobacco control cannot focus exclusively on cigarettes. These bans have been uneven in their implementation, and the products have sometimes re-entered markets through reformulation or under different branding. But the regulatory intent reflects a genuine understanding of the breadth of India’s tobacco problem.
Where the gaps remain most significant is in cessation support. India’s quit lines and counselling infrastructure, while growing, remain insufficient relative to the scale of tobacco use. Most tobacco users who want to quit do not have access to evidence-based cessation support — whether pharmacological, behavioural or a combination of both. Building this infrastructure, particularly in rural and underserved areas, is one of the most important unfinished tasks in India’s tobacco control agenda.
The Youth Crisis: A New Generation in the Crosshairs
Perhaps the most concerning development in global tobacco control in recent years has been the deliberate targeting of young people by tobacco and nicotine companies. This is not incidental. It is strategic. The industry understands that most long-term tobacco users begin before the age of 20, and that early nicotine dependence creates customers who are difficult to lose.
The vehicles for this targeting have changed. Traditional cigarette advertising, heavily restricted in most countries, has given way to a more sophisticated playbook. E-cigarettes and vaping devices marketed with bright designs, fruit and dessert flavours, and sleek aesthetics have been positioned as modern, lifestyle-compatible alternatives to traditional tobacco. Nicotine pouches, which are discreet and require no smoking or spitting, have expanded the accessibility of nicotine addiction to settings and populations that were previously harder to reach. Social media platforms where youth spend significant time and where advertising regulations are less consistently enforced have become primary channels for nicotine product promotion, often through influencer partnerships and content that does not look like advertising at all.
The WHO has noted that in countries with available data, adolescents are significantly more likely to vape than adults. It is the outcome of deliberate industry strategy. The flavours that make vaping products appealing — mango, mint, bubblegum, watermelon have no function other than to make nicotine delivery more attractive to people who might not otherwise try it. The packaging that resembles USB drives or makeup items has no function other than to reduce the social visibility of the act of using nicotine.
In India, the Electronic Cigarettes (Prohibition) Act of 2019 banned the production, import, sale and advertisement of e-cigarettes — one of the stronger regulatory responses to vaping in the developing world. But enforcement challenges remain and the products continue to circulate through informal channels and online platforms. The regulatory battle is an ongoing one and it requires consistent vigilance across multiple points of entry.
Anti-Tobacco Day 2026 is, in significant part, a call to protect this generation to ensure that the hard-won reductions in adult tobacco use are not undone by a surge in youth nicotine addiction dressed up in more appealing packaging.
The Environmental Cost of Tobacco: A Dimension Often Overlooked
Public discourse on tobacco tends to focus, understandably, on its health consequences. But the environmental cost of tobacco deserves attention as part of the complete picture.
Tobacco farming is resource-intensive and ecologically damaging. It requires significant quantities of pesticides and fertilisers, contributes to soil degradation, and has been associated with deforestation in tobacco-growing regions across Africa, Asia and Latin America. The curing of tobacco, the process by which harvested leaves are dried, traditionally requires large quantities of firewood, contributing to forest loss in countries where the crop is grown.
Cigarette butts are among the most common forms of litter found in global waste surveys. They are not simply paper and tobacco residue — they contain a plastic acetate filter that does not biodegrade, along with thousands of chemicals including nicotine, arsenic and lead, that leach into soil and waterways. The environmental persistence of cigarette waste is a public health problem in its own right, particularly in communities where water sources are vulnerable to contamination.
Recognising the environmental dimension of tobacco does not diminish the primacy of its health consequences. But it does expand the coalition of people and organisations for whom tobacco control is a relevant concern including environmental advocates, sustainable development practitioners and climate-focused policymakers.
The Role of Community Organisations: Where Policy Meets People
Legislation and enforcement are necessary but not sufficient. The communities most affected by tobacco — low-income households, rural populations, young people in under-resourced schools — are often the ones least likely to be reached by national awareness campaigns or healthcare services. This is where community organisations and NGOs play an irreplaceable role.
Smile Foundation’s Smile on Wheels programme illustrates what this kind of community-level work looks like in practice. Through mobile healthcare units that reach rural and underserved urban populations, the programme brings preventive healthcare, medical consultations, diagnostics, and health education to people who would otherwise have limited access to any of these. In communities where awareness of lifestyle disease risk — including the risks associated with tobacco — is low, this kind of sustained, trust-based engagement produces understanding that no poster campaign can replicate.
The integration of anti-tobacco awareness into existing community health programmes is one of the most effective ways to extend the reach of tobacco control. When a community health worker who is trusted and familiar raises the risks of tobacco use during a maternal health camp or a school health session, the message lands differently than it does from a government advertisement. It is personal, contextual and accompanied by the opportunity for questions and conversation.
Youth programmes that build leadership, critical thinking, and health literacy provide young people with the tools to recognise and resist manipulative marketing. Women’s health initiatives that address tobacco as part of a broader conversation about household well-being and economic security create connections between quitting and tangible benefits that abstract health messaging often fails to make.
The collaborative model — government policy and enforcement, civil society outreach and education, healthcare institutions providing cessation support — is the one that the evidence consistently points toward as most effective for sustained reduction in tobacco use.
The Case for Quitting: What the Evidence Shows
For current tobacco users, the message of Anti-Tobacco Day 2026 carries a specifically hopeful dimension. Quitting works, and the benefits begin sooner than most people expect.
Within 20 minutes of quitting, heart rate and blood pressure begin to normalise. Within 12 hours, carbon monoxide levels in the blood drop to normal. Within a year, the excess risk of coronary heart disease is half that of a continuing smoker. Within five years, stroke risk approaches that of a non-smoker. Within ten years, the risk of dying from lung cancer is approximately half that of a continuing smoker. These are not minor adjustments. They are significant, measurable improvements in health that occur at any age, after any duration of use.
The financial benefits compound these health gains. For a household spending a modest amount daily on tobacco, quitting creates savings that, over months and years, are meaningful — particularly in lower-income contexts where every rupee redirected from tobacco to food or education represents a real improvement in family well-being.
Quitting is difficult. Nicotine dependence is a genuine physiological condition, not simply a matter of willpower. The most effective cessation support combines behavioural counselling with pharmacological assistance — nicotine replacement therapy, prescription medications — and the kind of sustained social support that helps people navigate the periods of difficulty that accompany withdrawal. Expanding access to this kind of support, particularly in rural India, is one of the most high-impact investments that public health systems can make in tobacco control.
Anti-Tobacco Day 2026: What Each of Us Can Do
Anti-Tobacco Day 2026 is not only a policy conversation. It is a personal one.
For current tobacco users, it is an occasion to consider quitting, and to seek the support that makes quitting more likely to succeed. For parents and educators, it is a reminder to talk honestly with young people about nicotine marketing and the nature of addiction, before the industry gets there first. For employers, it is an opportunity to strengthen smoke-free workplace policies and to support employees who want to quit. For policymakers, it is a prompt to review the consistency of enforcement, the adequacy of cessation infrastructure and the regulatory gaps that the nicotine industry is actively exploiting.
For civil society organisations, Anti-Tobacco Day 2026 is a reminder that healthcare and education, delivered consistently and with genuine community engagement, are among the most durable forms of prevention available. The connection between community health programmes and tobacco control is direct, and organisations that already work with underserved populations are uniquely positioned to make it.
And for all of us, as citizens, as members of families and communities, it is a day to recognise that the choice to say no to tobacco, or to support someone else in making that choice, is part of something larger than individual health. It is part of the collective work of building communities, and a country, where health is valued over addiction, and where the industry that profits from harm does not get to set the terms of the conversation.
The Work That Continues
Anti-Tobacco Day 2026 arrives in a moment of genuine complexity. The progress made in tobacco control over the past two decades in legislation, in awareness, in declining smoking rates in many countries is real and worth acknowledging. So is the threat that the tobacco and nicotine industry’s reinvention represents. New products, new markets, new generations of potential users — the industry has not given up, and neither can the public health response.
India’s tobacco challenge is significant, but so is India’s capacity to respond — through law, through enforcement, through community health infrastructure and through the millions of people who have already chosen to quit or who are working to help others do so.
A tobacco-free future is not an abstraction. It is built, as most meaningful things are, through daily choices, sustained effort and the quiet work of education, healthcare and community connection. On 31 May 2026, the world once again makes its position clear. The work of making that position mean something continues every day after.
Frequently Asked Questions (FAQs): Anti-Tobacco Day 2026
What is Anti-Tobacco Day 2026 and when is it observed?
Anti-Tobacco Day 2026, officially known as World No Tobacco Day, is observed on 31 May every year, as an initiative led by the World Health Organisation. The day aims to raise awareness of the health, social, economic and environmental consequences of tobacco use, expose the tactics of the tobacco industry and encourage governments, communities and individuals to work toward a tobacco-free future.
In 2026, the official WHO theme is Unmask the Appeal: Countering Tobacco and Nicotine Addiction, with a particular focus on how the industry markets harmful products to young people.
What is the health impact of tobacco use globally?
Tobacco kills more than 8 million people every year, making it one of the leading causes of preventable death worldwide. This includes approximately 1.3 million non-smokers who die from exposure to second-hand smoke. Tobacco use is strongly associated with lung cancer, cardiovascular disease, stroke, chronic obstructive pulmonary disease and reduced immune function. Smokeless tobacco products carry additional risks including oral cancer, gum disease and oesophageal cancer. The global health burden of tobacco extends across nearly every organ system and affects users, their families and their communities.
How serious is tobacco use in India?
India is home to approximately 267 million tobacco users — one of the largest tobacco-using populations in the world. What makes India’s situation particularly complex is the diversity of consumption patterns, with significant use of both smoked tobacco — including bidis and cigarettes — and a wide range of smokeless tobacco products. Tobacco-attributable deaths in India exceed one million per year, and India accounts for a disproportionate share of global oral cancer cases, a direct consequence of high smokeless tobacco use. The economic burden is equally significant, with low-income households spending a substantial proportion of their income on tobacco at the direct expense of food, healthcare and education.
What laws govern tobacco control in India?
The primary legislative framework for tobacco control in India is the Cigarettes and Other Tobacco Products Act (COTPA) enacted in 2003. COTPA prohibits smoking in public places, restricts tobacco advertising across multiple media, bans sales near educational institutions and mandates health warnings on packaging. India has also implemented some of the world’s largest pictorial health warnings on tobacco packaging. The Electronic Cigarettes (Prohibition) Act of 2019 banned the production, import, sale and advertisement of e-cigarettes. The National Tobacco Control Programme supports enforcement, cessation services and public awareness at the state and district level.
Why is youth tobacco use a particular concern in Anti-Tobacco Day 2026?
The WHO has identified the deliberate targeting of young people by tobacco and nicotine companies as one of the most serious emerging threats in global tobacco control. E-cigarettes, nicotine pouches and flavoured devices — marketed with bright designs, appealing flavours and influencer-style social media promotion — are specifically designed to attract younger users who might not otherwise try tobacco products. In countries with available data, adolescents are significantly more likely to vape than adults. Anti-Tobacco Day 2026’s theme directly addresses this manipulation, calling on schools, families, governments and communities to protect young people from nicotine addiction before it begins.
What is the socio-economic impact of tobacco use?
The socio-economic impact of tobacco is significant at both the household and national level. For low-income families, spending on tobacco products directly competes with essential expenditure on food, education, healthcare and savings. At the national level, countries lose billions in healthcare costs and lost productivity due to tobacco-related illness and premature death. The environmental costs add a further dimension — tobacco farming contributes to deforestation and soil degradation, while cigarette butts are among the most common and environmentally persistent forms of litter globally, releasing toxic chemicals into soil and waterways.
What role do community organisations play in tobacco control?
Community organisations and NGOs play an irreplaceable role in reaching the populations that national awareness campaigns and formal healthcare systems do not consistently serve. Organisations like Smile Foundation, through programmes such as Smile on Wheels, bring preventive healthcare, medical consultations, diagnostics and health education directly to rural and underserved urban communities. Integrating anti-tobacco awareness into community health programmes — school health sessions, maternal health camps, youth leadership initiatives — allows tobacco education to reach people through trusted, familiar channels, making it significantly more likely to be heard and acted upon.
What are the benefits of quitting tobacco and how can people get support?
The health benefits of quitting tobacco begin almost immediately and compound significantly over time. Within 20 minutes of quitting, heart rate and blood pressure begin to normalise. Within a year, the excess risk of coronary heart disease is halved. Within ten years, the risk of dying from lung cancer is approximately half that of a continuing smoker. Financial savings, particularly meaningful for lower-income households, begin from the first day. For those who want to quit, the most effective support combines behavioural counselling with pharmacological assistance such as nicotine replacement therapy. In India, quit lines, hospital-based cessation clinics and community health programmes provide access to this support, though expanding these services, particularly in rural areas, remains an important priority.









3 replies on “Anti-Tobacco Day 2026: The World Says No, But the Fight Is Far From Over”
This is a very nicely designed website with useful content. Tobacco is a menace indeed. I am planning awareness campaign on similar lines. Would like to use some data from this article. Due credit will be given to you for excellent work being carried out on the slides. Thank you.
Dr. Ulhas Ganu
Dear Dr Ganu,
Thank you so much for your kind words—it really means a lot to us. We’re glad you found the website and content helpful.
It’s wonderful to hear that you’re planning an awareness campaign on tobacco. That’s such an important cause, and we truly appreciate the work you’re doing. Please feel free to use the data from the article—we’re grateful for your willingness to give credit.
Wishing you all the very best for your campaign.
Warm regards,
Team Smile Foundation
Thank you so much for the reply and allowing to use the material elsewhere, with due credit to you. The Diagrams and Figures speak so much. It should go a long way in convincing the people at large to quit smoking. Industrial units also should handle waste matter carefully to make reduce pollution.
Regards.
Dr. Ulhas Ganu