

For decades, development programming has treated women’s health, nutrition, and economic empowerment as separate verticals. Maternal health sits in one policy bucket. Nutrition in another. Livelihoods in a third.
On paper, this separation creates administrative clarity.
On the ground, it creates fragmentation.
A pregnant woman who is anaemic does not experience her life in verticals. Her health affects her productivity. Her productivity affects household income. Household income affects her child’s nutrition. Child nutrition affects cognitive development. And that development shapes the next generation’s economic trajectory.
If we are serious about advancing women’s well-being in India, we must move from fragmented interventions to integrated systems.
The Context: Persistent Gaps in Women’s Health and Agency
India has made measurable progress in maternal and child health over the last two decades. Yet structural gaps remain.
Recent studies highlight that only a minority of women receive comprehensive essential healthcare services. Meanwhile, over half of women of reproductive age continue to face anaemia — a condition that directly impacts maternal outcomes, productivity and economic participation.
Health and economic participation are not isolated realities.
Global research consistently shows that when women lack access to quality healthcare and nutrition, their labour force participation declines. Conversely, when women gain income and financial agency, health-seeking behaviour improves.
The relationship is circular, and reinforcing.
This is precisely why integrated models are no longer optional. They are essential.
Rethinking the First 1,000 Days
The first 1,000 days of a child’s life — from conception to two years of age — are widely recognised as critical for long-term physical and cognitive development.
But maternal health during this period is equally critical.
If a woman enters pregnancy anaemic, without access to antenatal care, and without adequate nutrition knowledge, the impact extends beyond delivery outcomes. It influences birth weight, early immunity and long-term growth trajectories.
Yet maternal health programmes often stop at clinical indicators.
What happens after childbirth? Does the mother regain nutritional stability? Does she have the agency to make health decisions? What about income security? Does she access government schemes? Does she have mobility to seek care?
These questions require a broader lens.
An Integrated Model for Financial Independence: Health, Nutrition and Enterprise
An emerging systems approach recognises that women’s well-being requires simultaneous strengthening of health services, nutrition behaviour and economic pathways.
Over the past year, the Swabhiman programme has demonstrated what this integration looks like in practice .
In FY 24–25:
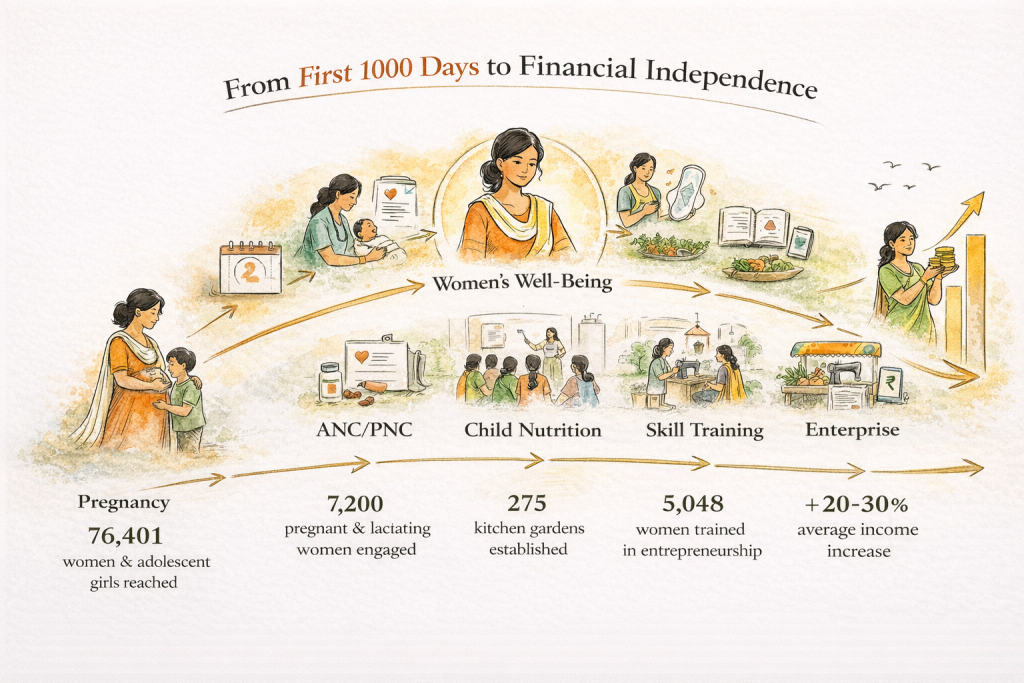
- 76,401 women and adolescent girls were reached with reproductive health education and healthcare services.
- 7,200 pregnant and lactating women and young children engaged in maternal and child health awareness.
- 68 women-led entrepreneurs were nurtured through structured business training and digital literacy.
- Over 1,90,000 total beneficiaries were reached across health and livelihood interventions.
These figures are not standalone achievements. They reflect a systems design.
Health awareness sessions are paired with entrepreneurship training. Nutrition counselling is reinforced through community kitchen gardens. Digital literacy supports access to teleconsultation services and financial inclusion.
Integration becomes reinforcement.
Strengthening Public Systems, Not Replacing Them
One of the most critical insights in development today is that sustainability depends on public system strengthening.
Parallel systems may produce short-term outcomes. Integrated systems produce long-term transformation.
The programme supported:
- Capacity building for 319 frontline workers.
- Strengthening of 7 Health and Wellness Centres.
- Refurbishment of 17 Anganwadi Centres.
- Deployment of teleconsultation services through government-linked platforms.
By investing in infrastructure, training, and convergence, the approach enhances the quality of public service delivery rather than substituting it.
This alignment with missions such as POSHAN Abhiyaan, National Health Mission, Skill India, and Digital India ensures policy coherence .
When women receive services through strengthened public platforms, continuity improves.
The Economic Agency Multiplier: Financial Independence
Health without income leaves women vulnerable. Income without health is unsustainable.
Through Entrepreneurship and Skill Training Programmes, women were trained in business planning, digital finance and enterprise management. International Labour Organization models such as GYB (Generate Your Business) and SYB (Start Your Business) were integrated into training frameworks.
The results were measurable:
- 5,048 women trained in entrepreneurship.
- 116 enterprises established.
- Average income increase of 20–30 percent among entrepreneurs.
Income increase is not merely financial. It shifts decision-making power.
When women contribute economically, household investments in education and nutrition often rise. Studies consistently confirm that women reinvest a higher proportion of earnings into family well-being compared to men.
Economic empowerment, therefore, feeds directly back into maternal and child outcomes.
Behaviour Change at the Community Level
Infrastructure and training alone do not shift norms. Behaviour change communication is essential.
Home visits, mothers’ meetings, and recipe demonstrations addressed diet diversity, breastfeeding, complementary feeding, hygiene and early pregnancy registration.
Over 24,500 nutrition snack boxes were distributed monthly for seven months, coupled with counselling for caregivers.
Meanwhile, 275 kitchen gardens were established to ensure local, low-cost access to nutrient-rich produce.
These interventions may appear small in isolation. Together, they reshape food environments.
When nutrition knowledge meets practical access, sustained change becomes possible.
Telehealth and Digital Convergence
Digital inclusion has opened new pathways for women in underserved geographies.
Teleconsultation services enabled women to access qualified doctors without travel constraints. Concerns related to maternal health, breastfeeding, and minor ailments were addressed in real time.
Digital literacy training supported use of UPI systems, savings platforms and government schemes.
The intersection of digital health and digital finance represents a significant opportunity for scale.
Women who can access telehealth, receive digital payments and market products online are positioned differently within their communities.
Adolescents: The Preventive Lens
If the first 1,000 days are critical, adolescence is transformative.
Menstrual awareness sessions, introduction of reusable sanitary napkins and adolescent reproductive and sexual health education aim to disrupt cycles of stigma and vulnerability.
Anaemia in adolescent girls is not merely a health statistic. It predicts future maternal risk, productivity loss and educational disruption.
Intervening early protects long-term trajectories.
Beyond Outputs: Qualitative Shifts
Quantitative achievements are necessary. But qualitative outcomes tell a deeper story.
Women reported:
- Improved awareness of reproductive and sexual health.
- Greater confidence in accessing services.
- Increased financial decision-making within households.
- Recognition of economic rights and gender equality.
Communities demonstrated stronger convergence between health departments, SHGs and local institutions.
A cadre of change agents emerged at the grassroots level.
These are the early markers of structural transformation.
Why Integration Matters for Policy
India’s policy architecture increasingly recognises convergence. Programmes such as RMNCHA+N, Anaemia Mukt Bharat and Skill India operate across health and livelihood domains.
However, implementation often remains siloed.
Integrated models demonstrate how convergence can function at the community level:
- Health workers trained alongside livelihood facilitators.
- Teleconsultations integrated with nutrition counselling.
- Enterprise development linked with digital financial inclusion.
- Infrastructure refurbishment paired with behaviour change communication.
Such models provide replicable frameworks for scaling through government platforms.
The Road Ahead: Scaling with Precision
Looking toward FY 25–26, the next phase involves deepening rather than merely expanding.
Priorities include:
- Sector-specific enterprise models and advanced business training.
- Expanded anaemia reduction campaigns aligned with national missions.
- Mobile medical units focused on women and adolescent girls.
- Tech-enabled monitoring for real-time case tracking.
Scale without precision risks dilution. Precision with scale creates transformation.
A Systems Future
Development discourse often celebrates individual success stories. These matter.
But systemic resilience requires integrated thinking.
Women’s health cannot be decoupled from economic participation. Nutrition cannot be separated from digital inclusion. Public infrastructure cannot be sidelined in favour of isolated interventions.
The pathway forward is clear:
From first 1,000 days to financial independence, maternal health to market access and from behaviour change to system strengthening.
When these elements converge, women do not merely survive. They lead.
And when women lead healthier, economically secure lives, communities move from vulnerability to vitality.
That is not a vertical solution.
It is a systems transformation.








